


Patients undergoing allogeneic hematopoietic cell transplant (HCT) for nonmalignant conditions may be at higher risk for post-transplant autoimmunity (AI). The precise risk factors for these events remain unclear.
Retrospective review was performed of 92 patients with primary immunodeficiency (PID) or immune dysregulation who received HCT at our institution between 2000 and 2024.
17 of 92 patients (18%) developed AI at a median of 9 months post-HCT (HCT details in supplementary table 1; AI details in supplementary table 2). Majority received our institutional standard Bu2/Flu/ATG conditioning. There were no differences in primary diagnosis, donor type, graft source/composition, conditioning, or rates of graft-versus-host disease (GVHD) between AI and non-AI patients. Hematology AI diagnoses were most common. Antibody-positive rheumatologic disease was reported in 3 patients: mixed connective tissue disease (MCTD) with erosive arthritis, systemic lupus erythematous (SLE)/juvenile idiopathic arthritis (JIA) overlap, and immune-mediated necrotizing myositis. Patients with severe combined immunodeficiency (SCID) were overrepresented in the non-hematologic AI group (heme SCID = 1, nonheme SCID = 6). There was no relationship between immunosuppressive therapy (IST) and development of AI: 11 patients off IST and 6 on IST at time of AI diagnosis. Of AI patients, 14 (82%) developed an infection by day (D) 100 compared to 49 non-AI patients (65%; p = 0.17). Of AI patients, 24% developed acute GVHD (all skin GVHD), and one patient developed limited skin chronic GVHD; these patients all developed hematologic AI. Patients who required cell boost or second HCT were more likely to develop AI: 4 AI patients (24%) vs. 8 non-AI patients (11%, p = 0.16). Two of three AI patients requiring repeat intervention later developed rheumatologic disease. AI events were not associated with subsequent decline in chimerism (Fig. 1). One patient experienced a drop in chimerism >20% following AI event. AI patients were less likely to achieve CD4+ >50 cells/μL by D+100 and CD19+ >200 cells/μL by D+360 than non-AI patients (CD4+: AI 65% vs. non-AI 89%; CD19+ AI 59% vs. non-AI 89%).
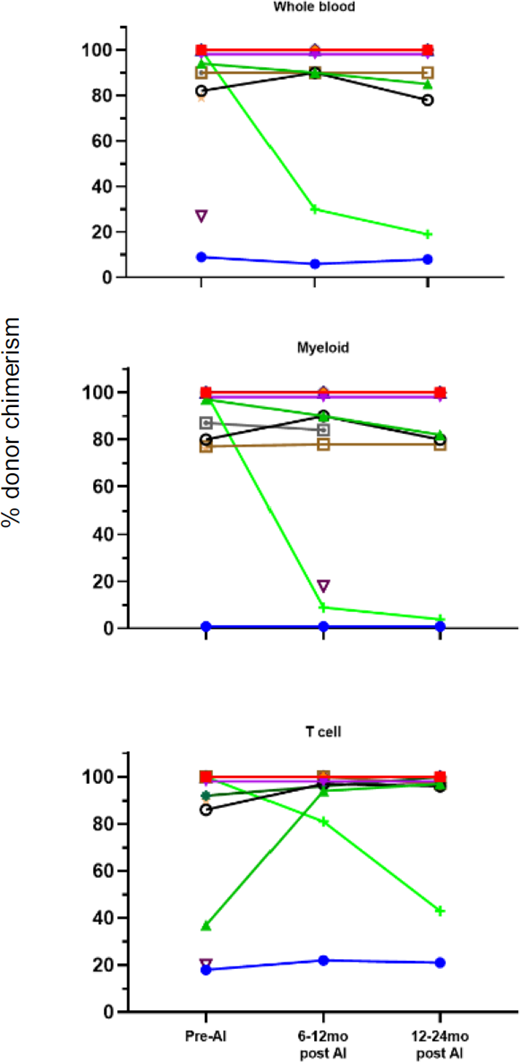
Donor chimerism pre- and post-AI diagnosis.
We report post-HCT AI of 18% in our PID/immune dysregulation population, including multiple patients with rheumatologic AI manifestations. We saw no impact of graft source, donor type, GVHD, or post-HCT immunosuppression on development of an AI complication. Patients with infection by day 100 were likely to develop post-HCT AI, which may be related to early immune activation. Second intervention increased risk of developing AI. Further studies are needed to determine if this is related to extensive immune system modulation or predisposition to both post-HCT AI and graft rejection.


