


Common variable immunodeficiency (CVID) is characterized by recurrent infections due to impairments in antibody quantity and quality. As such, immunoglobulin G replacement therapy (IgGRT) is the standard-of-care (SOC) for CVID patients. However, national patterns of IgGRT use and variations in SOC receipt rates among demographic groups remain poorly characterized. Furthermore, there is a limited understanding of how disease burden evolves across age and gender at a cohort level.
Quantifying SOC receipt rates and characterizing the longitudinal disease progression are essential for identifying care variations and detecting high-risk disease accumulation points.
We aimed to quantify regional and racial differences in IgGRT utilization among CVID patients and to characterize longitudinal patterns of disease progression. We identified CVID patients within the TriNetX electronic health record (EHR) dataset via ICD-9/10 diagnostic codes. IgGRT receipt was defined as a binary SOC outcome and compared across U.S. regions (Midwest, West, Northeast, South, and other) and self-reported racial groups (White, Black, Asian, and other). We calculated multivariate logistic regression estimated odds ratios (ORs) with 95% confidence intervals (CI) to assess demographic differences in treatment receipt rates. To evaluate longitudinal disease progression, the cohort was stratified by age and gender, followed by the enumeration of cumulative disease categories over time.
White patients in the West had significantly higher odds of receiving IgGRT than White patients in the South (OR = 1.47, 95% CI: 1.33–1.63, p < 0.05), whereas Black patients in the Northeast had markedly lower SOC achievement odds (OR = 0.45, 95% CI: 0.31–0.65, p < 0.05) (Figure 1). Trajectory analysis showed distinct age- and gender-dependent patterns: females exhibited higher cumulative disease burden by ages 50–60, while males demonstrated increased burden in early childhood and in mid-adulthood (Figure 2). Across both genders, respiratory diseases and immune-related abnormalities increased substantially by age 50–60.
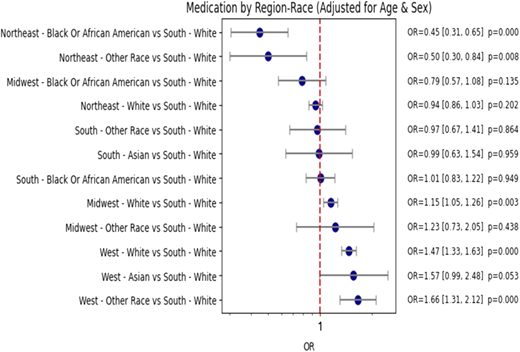
Adjusted odds ratios (OR) for medication (IgGRT) receipt by region-race for the CVID cohort, shown with 95% confidence intervals.
Adjusted odds ratios (OR) for medication (IgGRT) receipt by region-race for the CVID cohort, shown with 95% confidence intervals.
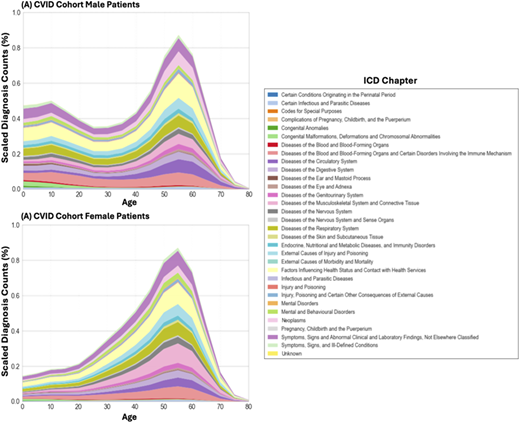
Density plots stratified by age and gender, indicating disease trajectories for (A) CVID cohort.
Density plots stratified by age and gender, indicating disease trajectories for (A) CVID cohort.
Using a U.S. national EHR-based analysis, we demonstrate significant demographic differences in IgGRT utilization and disease progression patterns among individuals with CVID. We have noted that these patterns indicate that CVID disease burden follows gender-specific trajectories early in life but accumulates by age 50–60. These findings inform the need for time-based intervention strategies to reduce treatment gaps, improve detection, and reduce morbidity.


