

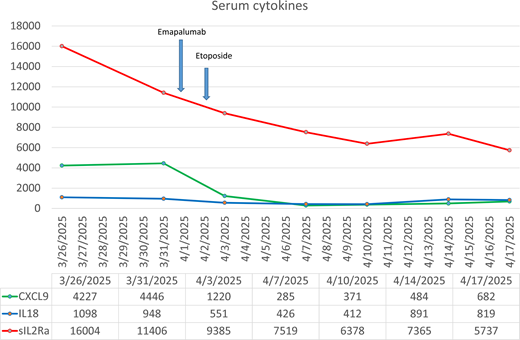
A 12-day-old full-term (FT) male presented with one day of diarrhea and respiratory distress. The exam was notable for hypothermia, tachycardia, and hypoxemia. Initial bloodwork showed leukopenia (3,400 cells/uL, absolute neutrophil count [ANC] 710 cells/uL, absolute lymphocyte count [ALC] 1,460 cells/uL), thrombocytopenia (56 cells/uL), C-reactive protein (CRP) >19, procalcitonin 5.2, hyponatremia (126), and hypoalbuminemia (2.0). Chest x-ray revealed bilateral patchy opacities. Broad-spectrum antibiotics were initiated, and an extensive infectious workup was unrevealing. Within 24 hours, he required extracorporeal membrane oxygenation. On day 4, plasmapheresis was initiated. A reticular non-blanching rash developed. Intravenous (IV) methylprednisolone and IV immunoglobulin (IVIG) were started. Quantitative immunoglobulins and complements were normal. Lymphocyte subsets (CD3/4/8/19/56) showed a global reduction in absolute counts. Cytokine testing was notable for: CXCL9: 4,227 (ref:<769 pg/mL), IL-18: 1,098 (ref:82-344 pg/mL), IL-2RA, soluble: 16,004 (ref:325-1,785 pg/mL), IL-6: 6,407 (ref:<=9), IL-8: 10,505 (ref:<=7), and INF-y: 7 (ref:<=1) (Figure 1). Whole genome sequencing (WGS) identified a maternally inherited hemizygous variant of uncertain significance (VUS) in dedicator of cytokinesis 11 (DOCK11) c.4096 C>T p.(R1366W), predicted to be deleterious on in silico analysis (Figure 2). Treatment was escalated to anakinra, emapalumab, and etoposide with serologic improvement (Figure 1) and rash resolution. Legionella was identified on blood culture through Matrix-Assisted Laser Desorption/Ionization-Time of Flight (MALDI-TOF) and confirmed with bronchoalveolar lavage (BAL). A second treatment course of levofloxacin was initiated, but unfortunately, his lung disease progressed with diffuse alveolar hemorrhage. Extracorporeal membrane oxygenation (ECMO) complications required premature decannulation and ultimately death.
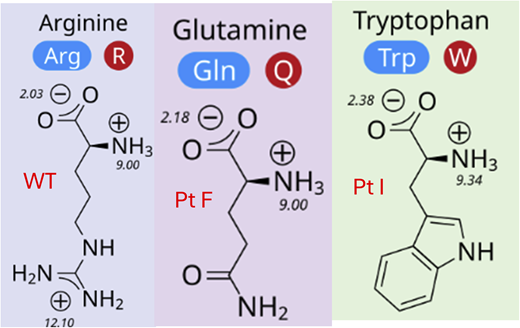
The first panel is the WT amino acid (AA) at 1336. The second panel is a patient reported with a pathogenic variant leading to AA substitution with glutamine, a similarly sized polar uncharged amino acid. The third panel is our patient, with a variant leading to AA substitution with tryptophan, a larger and hydrophobic AA.
The first panel is the WT amino acid (AA) at 1336. The second panel is a patient reported with a pathogenic variant leading to AA substitution with glutamine, a similarly sized polar uncharged amino acid. The third panel is our patient, with a variant leading to AA substitution with tryptophan, a larger and hydrophobic AA.
DOCK11 is an activator of CDC42, a central regulator of actin cytoskeleton dynamics in hematologic cells. DOCK11 deficiency is an actinopathy resulting in impaired hematologic cell structure and function. Fewer than 20 cases have been reported. Complete loss of function is associated with a severe autoinflammatory phenotype and high-mortality risk. Partial loss-of-function is associated with polyautoimmunity and early-onset inflammatory bowel disease (IBD). Legionella is an extremely rare opportunistic organism in the first few months of life, even in those with immunodeficiency or structural lung disease. However, Legionella is an intracellular pathogen and inhibits the actin cytoskeleton. This double hit may have resulted in persistent disseminated infection and the state of cytokine storm.



