


Chronic norovirus infection (CNI) is a significant cause of morbidity and mortality in immunocompromised patients. We sought to determine clinical and virologic features associated with CNI with an emphasis on IEI.
Norovirus-positive stool samples from 88 patients at the NIH Clinical Center from 2010 to 2023. Longitudinal clinical and virologic data were collected.
Forty-eight patients had CNI; 23 had acute norovirus infection (ANI); 17 patients were unclassifiable. Eighty-three percent of CNI patients had an underlying diagnosis of IEI, including CID (N = 23), CVID (N = 11), and SCID (N = 6). The majority with ANI had hematologic disorders (48%); only 5 (21%) had CVID, CID, or SCID. Mortality in the CNI cohort was 38%. More than half of CNI patients had nutritional defects, including electrolyte abnormalities and hypovitaminosis; 20% required TPN. GII.4 was the predominant norovirus genotype among all patients, although diverse genotype I and II viruses were represented. Gastrointestinal coinfections during CNI infection were prevalent (50%); the most common being enteropathogenic E. coli (N = 12) and C. difficile (N = 12).
Seventy-seven percent of CNI patients had chronic liver disease, including both cholestatic (N = 18) and hepatocellular (N = 14) patterns. Thirty-three percent (N = 16) of CNI patients had a diagnosis of nodular regenerative hyperplasia (NRH). Only 35% of patients with ANI had chronic liver disease.
Twelve patients with CNI eventually cleared norovirus (median duration of 688 days versus 18 days for ANI). Eight patients cleared in the setting of definitive immune reconstitution, specifically HSCT or gene therapy. Three patients cleared in the setting of immunomodulatory therapy for concurrent IEI-related enteropathy treated with ustekinumab, abatacept, and/or JAK inhibitors. No patient cleared after traditional CNI therapies, including nitazoxanide, ribavirin, or immunoglobulin (PO or IV).
CNI patients were nutritionally compromised with high mortality and a high prevalence of liver disease. IEI with adaptive defects were disproportionately represented in CNI. Common CNI treatments were not effective. CNI consistently resolved with definitive immune reconstitution; some patients cleared infection with immunomodulatory therapy for enteropathy, suggesting a new treatment strategy to be explored in future studies. To our knowledge, this is the largest cohort of CNI with a focus on IEI analyzed to date.

Category of underlying diagnosis.
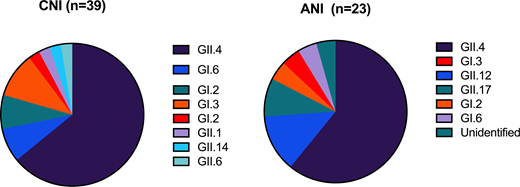
Norovirus genotypes represented across cohorts.


